


- Abnormal bronchoesophageal communication due to carcinoma of the esophagus.
- Bronchoesophageal post-traumatic communication.
- Bronchial stenosis.
- After the resection of the carcinoma in a source bronchus.
- Traumatic bronchial rupture.
The Stening® Cone MD Stent can be inserted with a large bronchoscope or with an applicator.
If an applicator is available, it consists of two telescopic metal tubes of different lengths.
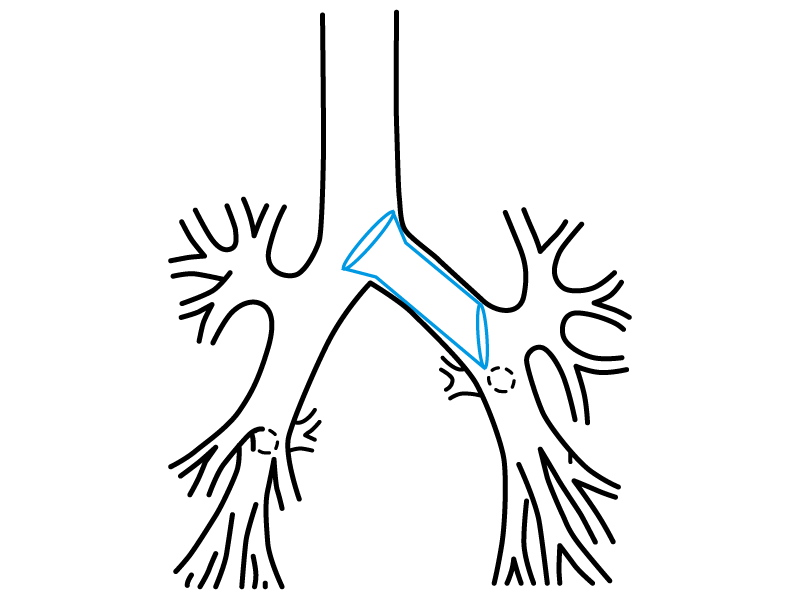
Insert the optics inside the applicator, then collocate the Stening® Cone MD Stent at the end of the applicator, as shown in the photograph. The bevelled end of the Cone should be on a distal position and oriented so that its oblique end faces the entrance of the superior bronchial lobe.
Perform the orotracheal intubation with the optical-introducer-Stening® Cone Stent assembly, under direct endoscopic vision. Move towards the affected source bronchus, guiding the assembly inside the trachea until you reach the source bronchus. When you reach the affected area, advance until you surpass the distal end of the fistula or bronchial injury over one centimetre.
Then, keep the external tube of the introducer immovable and gently remove the internal one together with the optics.
The Stening® Cone Stent will be released inside the bronchus. Remove the applicator and intubate the airway again with a conventional bronchoscope to perform an inspection.

- Maintain the moisture of secretions, whenever they appear, by taking nebulisations frequently with a warm isotonic saline solution.
- Perform a periodic check-up following your doctor’s advice.
The product should not be reused because this can cause cross contamination.
