Endoscopy Section, Pulmonology Division, Hospital Dr. E. Tornú – Buenos Aires
Abstract
Objective
Presentation of airway recanalization in 300 patients in the Respiratory Endoscopy section of Hospital Tornú: 115 women (38.33%) and 185 men (61.66%), aged between 14 and 86 years. Mean age 52 ± 16.26.
Material
Reports of interventional bronchoscopies performed to treat 300 patients with total or partial airway obstruction due to lesions of benign or malignant nature, carried out in the period 9/15/1997 to 1/1/2010. Patients who met recanalization criteria were included: those presenting a benign tracheal stenosis with reduction of the lumen to a diameter equal to or less than 8 mm; all cases of benign bronchial stenosis affecting 50% of the lumen; and patients with endo-tracheobronchial tumors that occluded 50% or more.
Cases were excluded in which open surgical treatment was possible, those that presented involvement of the pulmonary parenchyma or of the bronchial lumen distal to the obstruction, and patients with pleural effusion or atelectasis of more than two months' evolution.
Results
388 therapeutic procedures were performed and recanalization of the airway was achieved in 96.33% of cases. Tolerance to the stents was 99.68%, and 100% for the metal-free silicone prostheses. The complication rate was 6.32%, with hemorrhage in first place. The mortality attributable to the treatment was 0.25%.
Conclusions
Rigid bronchoscopy restored the lumen in airway obstructions with a success rate above 96%. Silicone prostheses with stenotic designs are more effective than straight models for the treatment of benign tracheal stenoses.
Introduction
The endoscopic treatment of lesions that produce occlusion or subocclusion of different magnitude in the trachea, main bronchi or some lobar bronchi has achieved sufficient diffusion within the international medical community, to the point that its performance is well established (1). The indication to apply a method that can recover the pulmonary ventilation suspended by the presence of an obstructive lesion arises immediately in the bronchoscopist. However, it has remained limited to those cases in which open exeresis treatment is not possible. The use of silicone endoprostheses is another widely used resource in order to provide additional support to the airway after treatment and to prolong its effectiveness. Thus, endosurgical treatment has been simplified and interventional physicians have accumulated experience in its performance, a task that has shown to provide benefits proportional to the magnitude of the difficulties overcome during its implementation (2, 3).
Material and methods
Data were obtained retrospectively from the interventional bronchoscopy reports corresponding to procedures performed to treat 300 patients, with benign and malignant conditions that partially or completely occluded the large airway. The interventionism applied to the patients was performed in one or several sessions. None of them was amenable to resection treatment by conventional surgery, and all underwent a flexible bronchoscopy in order to evaluate the characteristics of the lesion. Thus, the indication for the procedure was maintained considering the possibility of pulmonary re-expansion and the clinical presumption of improving the dyspnea with treatment, in all cases of malignant disease and in benign stenoses that reduced the lumen by 50% or more. This subjective evaluation was established by comparing the diameter in the affected area with that existing in the healthy airway near the lesion, and with the reference of the known caliber of the bronchoscope in use. The patients underwent treatment with a rigid or flexible bronchoscope, under general anesthesia and muscle relaxation, in the operating room and under continuous control of cardiac and respiratory function. They received 2 grams of intravenous cephalothin in rapid injection minutes before the procedure. The treatments were carried out by two experienced pulmonologists, with exclusive dedication to bronchoscopy. For airway recanalization, dilation maneuvers were performed with bougies of increasing diameter, balloon and/or rigid bronchoscope. An electrocautery was also used to make cuts in some benign stenoses and thermocoagulation with tissue vaporization in malignant lesions. The cases, for the most part, were treated using a rigid bronchoscope with interchangeable tubes of different calibers, a set of optics, prosthesis introducers, forceps suitable for their mobilization, probes and tapes for the application of Montgomery-type T-tubes. In a few cases, the treatment was performed or completed with an Olympus BF1T30 flexible bronchoscope. The application of different models and dimensions of silicone airway stents was arranged, although dynamic and self-expandable stents were also used. Tolerance to the prosthesis was defined as the absence of symptoms attributable to them that motivated their removal. Therapeutic success was defined as the restitution of the tracheobronchial lumen: in the benign stenoses, it was established to determine as satisfactory tracheal or bronchial recanalization all those in which the lumen of the affected area had reached 75% or more of the normal caliber for that case, after the end of treatment. Immediate complications were considered to be all those situations attributable to the procedure (hemorrhage, desaturation with a decrease greater than 4%, rupture of the airway wall, stent migration) occurring during and up to 48 hours after it was performed. Cases of death were recorded when it was due to the instituted treatment or a direct consequence of it, during its application or afterward.
Results
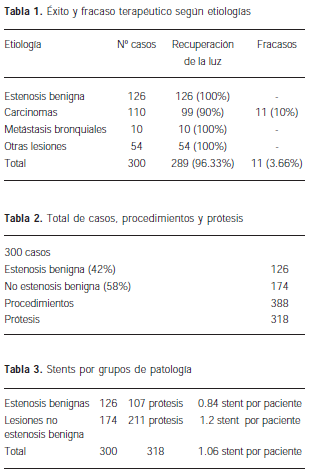
388 procedures were performed in 300 patients (1.29 procedures per patient). Those performed with a rigid bronchoscope totaled 383 (98.7%), while in 5 cases the flexible bronchoscope was used (1.3%). In 11 of the 300 cases, recovery of the bronchial lumen was not possible and it was then considered a failure of the procedure. All of them corresponded to patients with a diagnosis of carcinoma, and the endobronchial tumor lesion was also intramural and infiltrating. Airway recanalization was possible in 289 patients (96.33%) (Table 1).
Of the total, 115 were women (38.33%) and 185 men (61.66%), in an age range of 14 to 86 years. The mean age was 52 ± 16.26 years and, for the treatment, 311 silicone prostheses (97.8%), one polyflex® self-expandable stent and 6 Freitag dynamic prostheses were used, adding up to a total of 318 devices. In this way, 126 benign stenoses in the trachea and bronchi (42%) and 174 "non-benign-stenosis" conditions (58%) were treated (Tables 2, 3). This last group comprises 110 cases of carcinomas that include 10 metastases of extrapulmonary primary tumors.
As for the use of prostheses by pathology, the 126 benign stenoses required 107 stents for their treatment (0.84 stents per patient).
For the group of "non-benign-stenosis" lesions, of 174 cases, 211 devices were used (1.2 ± 4.6 prostheses per patient) (Table 3).
In 51 of the 300 cases treated, no prostheses were used in the first therapeutic session. Of these, 11 correspond to the benign stenosis group and 40 to the non-benign lesion group. Of the latter, 32 cases in which a stent was not used initially had malignant tumor disease.
Of the 388 procedures, complications occurred in 44 of them (11.34%), which will be detailed below.
Benign stenosis group
Of the 126 cases with benign stenosis, 122 affected the trachea (96.82%) and 4 (3.18%) the main bronchi. 100 of the total (79.40%) were post-intubation stenoses. Of the remaining 26, 4 occurred at the site of a previous tracheostomy, 4 were recurrences at the site of an end-to-end anastomosis from open surgery previously performed for the resection of the tracheal stenosis, 4 following tracheal rupture, one after severe laryngeal trauma and another due to aortic aneurysm. The cause could not be determined in 9 cases.
Four benign stenotic lesions were in the main bronchi: two were sequelae of pulmonary tuberculosis, one following traumatic bronchial injury and another following anesthetic bronchial intubation. The tracheal stenoses were of complex conformation in 113 cases (89.7%), simple in 11 (8.7%), and 2 were subglottic (1.6%) (Table 4).

"Non-benign-stenosis" group
The group of patients not included with the benign stenoses is made up of all the cases that presented other invasive lesions of the tracheobronchial lumen or that developed their growth in it; and although it is composed in greater number of bronchial carcinomas, other etiologies were also found in this set, and none of them, as mentioned, can be included in any way with the benign narrowings that affect the airway.
Thus, this group includes 174 patients, of whom 38 had their condition located in the trachea, 101 in the bronchi and 35 shared both locations. Table 5.
In 11 (10%) of the 110 cases of carcinoma, reconstruction of the tracheal or bronchial lumen was not possible (Table 1).
As for the histological type of the lesions, 28 epidermoid carcinomas, 25 adenocarcinomas, 10 small-cell carcinomas, 2 giant-cell carcinomas and 8 carcinoid tumors were found. The endobronchial metastases totaled 10 cases. In another 13, the endoscopic biopsy identified the carcinoma but was not sufficient to establish its histology.
In addition, 1 chondroma, 1 neurofibroma, 11 esophageal carcinomas that invade the bronchial, tracheal or both lumens; 7 thyroid carcinomas involving the tracheal wall, 4 mediastinal tumors and 1 lymphoma were found. In one case the diagnosis was papilloma, in another leiomyosarcoma, 1 granuloma and 2 bronchial amyloidoses. In a further 45 cases the diagnosis could not be established by flexible bronchoscopy, and they were equally subjected to endoscopic disobstruction treatment. Epidermoid carcinoma was the most frequent tumor with 25.45% of cases, followed by adenocarcinoma (22.72%) and oat cell (9.09%) (Table 6). In this group, 211 prostheses were used for 174 patients (Table 3).
Three patients with bronchopleural fistula also received bronchoscopic treatment, in whom the fistula was blocked with a cylindrical, solid silicone device.
In relation to the 10 metastases, 8 of them were from clear-cell renal carcinoma, one from a breast tumor and the other from the colon (Table 7).
Complications occurred in 11 cases (6.32%), led by hemorrhages that equaled the suction capacity of the aspiration system; 3 in total (1.71%) resulted from the treatment of a non-typified carcinoma, an adenocarcinoma and a carcinoid tumor.

The complications of the present "non-benign-stenosis" group of lesions continue with a case of intense mucosal edema at the end of a dynamic stent (0.54%), reversible cardiac arrest during the treatment of a tracheal rupture (0.54%); a superior vena cava syndrome (0.54%) followed by death at 48 hours in a patient with adenocarcinoma that invaded the trachea and both main bronchi (0.54%), an atrial fibrillation in a case with adenocarcinoma (0.54%) and a partial pneumothorax in a patient lacking histopathological diagnosis.
Thus, the mortality determined for this group of 300 patients is 0.33%, and considering the mortality linked to the procedure, it is reduced somewhat more, to 0.25% (Table 8).
Intolerance to the prosthesis turned out to be extremely rare. It was only observed in one case in the entire series, representing 0.33% in relation to the treated patients and somewhat less, 0.31%, if considered in terms of the stents used.
It is a dynamic "Y" prosthesis implanted in a patient with intrabronchial metastasis of a primary clear-cell renal tumor. The intolerance, manifested by intractable coughing, was attributed to the intimate contact of the proximal end of the prosthesis with the tracheal mucosa adjacent to one of its rings. The stent was shortened and reinstalled without symptomatic relief and had to be removed and replaced.
Discussion
The usefulness of the method is well consolidated and the selection of patients has been widely commented on and published. Thus presented, the debate on these points would be, given its lack of novelty and the even smaller contribution of knowledge, monotonous and unnecessary. Observing the frequencies of appearance of problems, or the lack of them, considerations arise that are the start of this discussion. The series of 300 cases contains a numerous group of benign stenosis, mostly tracheal. In all of them the caliber of the airway was recovered with endoscopic interventionism. So the procedure in general was clearly satisfactory, with a success in achieving its purpose of 96.33%. Having announced electrocautery as the only cutting, vaporization and thermocoagulation device used in this series, its resolution capabilities bear an obligatory relation to the 96.33% of resolved cases (4-6). The 3.66% of failures corresponds to 11 cases with diagnoses of carcinoma. In them, the procedure fails to find the lumen distal to the airway obstruction (5), as happens when the lesions turn out to be intramural and highly infiltrating, that is, when the sought-after lumen does not exist. The analysis of the "non-benign-stenosis" group revealed, first, a greater quantity of prostheses used (211 units), and its cause is found in the need to use more than one stent per patient and also in having required more than one procedure per patient. This in turn indirectly shows that the probable extension of survival allows the malignant disease to progress and, with it, to recur by obstructing the airway at the same or a different site, motivating a new intervention. Most of the cases in this group suffered from carcinomas, bronchopulmonary or of neighboring organs. Among the latter, that of the thyroid, with locoregional extension and invasion of the tracheal lumen, a circumstance and etiology that in no way modifies the bronchoscopist's conduct. Eleven cases of esophageal carcinoma which, unlike the previous one, damages and breaks through the posterior wall of the trachea or, when its location is lower, involves the left main bronchus, again on its posterior wall, since it is there that the esophageal path crosses this bronchus. Often the damage is of left para-carinal location, with the esophagus coming to occupy the bronchial lumen. To endoscopically realign the left main bronchus, displace the esophagus and cover the fistulas that are a frequent companion in this picture, the use of a smooth-walled silicone stent has been very useful, since anchors are not necessary in this circumstance. One of the ends of the device widens in the shape of a cone and coincides anatomically with the origin of the main bronchus. The distal end is beveled and, by its shape, makes the maneuver of entering the bronchus and introducing the stent simple.

Migration of the prostheses, although less common in malignant conditions, is also possible. Only two migrations (1.49%) are described here, one of which corresponds to a carcinoid tumor in which an error in the early typing of the lesion led to the treatment of the obstruction with stent implantation. Few comments will be made about two fortunately infrequent facts, such as intolerance to the stent, whose reasons have already been clearly developed; and death as a result of the procedure, which in our report was 0.25%. It corresponded to a patient with mediastinal disease due to an adenocarcinoma. Since the mediastinal syndrome makes rigid bronchoscopy risky for diagnostic purposes, this risk will be reasonably increased when the procedure is also therapeutic, since the same factors that operate in the first will be more influential in the second, because the time necessary for the intervention will be, for easily understandable reasons, much greater. Thus, the maneuvers it entails and the displacement of tissues caused by the rigid bronchoscope lead to an increase in local inflammation and a worsening of the already compromised venous return to the mediastinum. Such was the case in ours.
References
- Cavaliere S, Venuta F, Foccoli P, Tonielli C, La Face B. Endoscopic treatment of malignant airway obstructions in 2008 patients. Chest 1996; 110: 1536-42.
- Stephens K E, Wood DE. Bronchoscopic management of central airway obstruction. J Torac Cardiovasc Surg. 2000;119:289-96.
- Dumon JF, Dumon MC. Dumon-Novatech Y-Stents: A Four-Year Experience with 50 tracheobronchial Tumors Involving the Carina. J Bronchol 2000; 7:26-32.
- Sutedja, T. Endobronchial electrocautery is an excellent alternative for Nd-YAG laser to treat airway Tumors. J of Bronchology 1997;4:101-105
- Boelcskei PL, Dierkesmann R, Bauer PC, Becker HD, Bolliger CT, Wolfgang FJ. Section on respiratory endoscopy of the German Society of Pulmonology. Recommendations for bronchoscopic treatment of tracheobronchial occlusions, stenoses, and mural malignant tumors. J Bronchol. 2000;7:133-8.
- Huisman C, van Kralingen KW, Postmus PE, Sutedja TG. Endobronchial Lipoma: A Series of Three Cases and the Role of Electrocautery. Department of Pulmonology, Academic Hospital Vrije Universiteit, Amsterdam, The Netherlands. Respiration 2000; 67: 689-92.