Case description
This is a 29-year-old male patient. He was hospitalized for severe traumatic brain injury and underwent orotracheal intubation for mechanical ventilation. On day 8, a tracheostomy was performed and he continued on mechanical ventilation for a total of 21 days. He remained with a nasogastric tube for three weeks.
After extubation, symptoms of tracheal aspiration appeared (coughing and expectoration after intake) and a tracheoesophageal fistula was suspected. Flexible bronchoscopy (FBC) was not conclusive in determining the existence of the fistula. A rigid bronchoscopy was performed in which parallel and asymmetric longitudinal folds and grooves are observed on the posterior tracheal wall, three centimeters distal to the stoma of the recent tracheostomy.
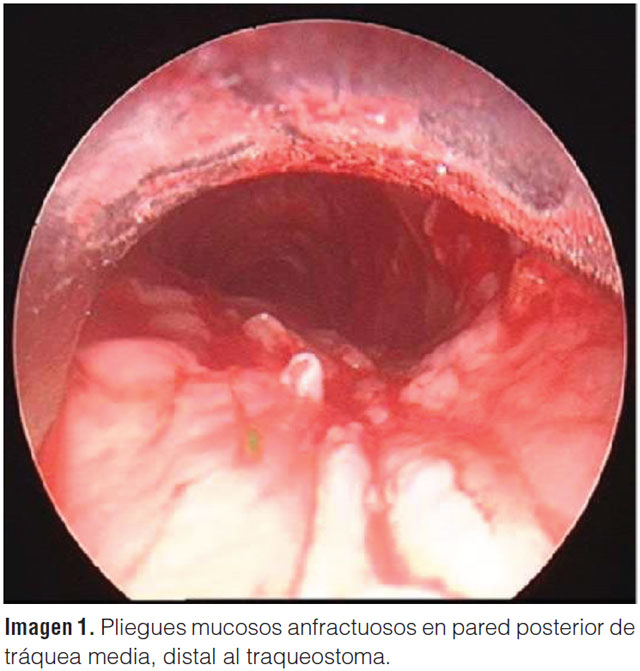
The intense edema with mamillated areas conceals the plane of the mucosal surface and does not allow detecting the existence of a communication, much less a formed fistula.
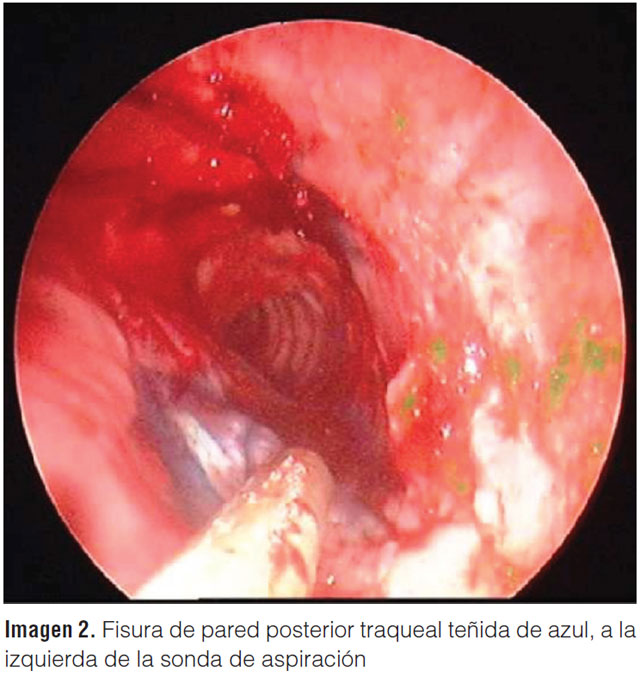
A diluted solution of methylene blue was instilled into the esophagus.
To the left of the suction catheter and in the center of the photograph, a pale area is observed on the posterior wall, furrowed by a thin, linear and winding tract stained by the methylene blue. Fissure of the posterior wall with demonstrated esophageal communication.
Discussion
Acquired tracheoesophageal fistula (TEF) is a rare complication that can occur for multiple reasons. The most common non-neoplastic etiology is the one related to complications of orotracheal intubation and tracheostomy. In general, they are attributed to tracheal injury caused by the cuff, in addition to underlying clinical conditions. This complication is generally iatrogenic and occurs in less than 1% of patients. The new devices with low-pressure cuffs have made this complication infrequent; however, it is a serious clinical situation with high morbidity and mortality1.
TEF should be suspected in risk situations. Most patients under mechanical ventilation (MV) present increased secretions, pneumonia and evidence of aspiration of gastric contents. When it is diagnosed after extubation, the most frequent sign is “coughing after liquid intake”; as the patient presented2.
The diagnosis is made by bronchoscopy and esophagoscopy. Other detection techniques have been described for patients under MV, such as observation of the gastric bag in different phases of the respiratory cycle (the “breathing bag”) or analysis of gases in this same bag, considering the passage from the airway of air with high oxygen concentrations3.
Direct bronchoscopic visualization of the site often reveals the wall defect. The presence of larger or smaller air bubbles also helps to locate the site. This allows a definitive diagnosis to be made. In the case of our patient, the intense edema of the lesion on the posterior wall of the trachea prevented confirming or ruling out this suspicion. An old and classic “Methylene Blue test” was useful in locating the fistula. Shah et al. described the usefulness of its use in a case report, in a patient with a tracheal stent4. Benatta et al. also reported its use in a case of persistent TE fistula after surgical correction of esophageal atresia in a two-month-old infant5. However, the use of methylene blue should be prudent, since it can be replaced by less toxic substances such as the cake dye used in confectionery (cake blue). Methylene blue is a potent inhibitor of monoamine oxidase (MAOI) and its intravenous use could trigger serotonin syndrome in patients using certain types of antidepressants6.
In general, the treatment is deferred surgery after prior defunctionalization of the area, once the critical conditions of MV, bronchoaspiration and nutritional status of each particular case have been overcome. Correct diagnosis is crucial in the evolution of these patients.
Conflicts of interest
The author declares that he has no conflicts of interest.
References
- Reed MF, Mathisen DJ. Tracheoesophageal fistula. Chest Surg Clin N Am 2003; 13(2): 271-89.
- Mooty RC, Rath P, Self M, Dunn E, Mangram A. Review of tracheo-esophageal fistula associated with endotracheal intubation. J Surg Educ 2007; 64(4): 237-40.
- Shah A, Ost D, Eapen GA, Morice RC, Jimenez CA. Diagnostic methylene blue test for stent covered tracheoesophageal fistula. Am J Respir Crit Care Med 2012; 185 (7): 9.
- Hasselbacherm DA, McCormick J. Tracheoesophageal Fistula: an Uncommon Cause of Ileus and Diagnosis Via Gastric Air Analysis. Chest 2006; 130: 286S-c-287S.
- Benatta MA, Benaired A, Khelifaoui A. Endoscopic stenting and clipping for anastomotic stricture and persistent tracheoesophageal fistula after surgical repair of esophageal atresia in an infant. Case Rep Med 2014: 738981.
- Ramsay R, Dunford C, Guillman PK et al. Methylene blue and serotonin toxicity: inhibition of monoamine oxidase A (MAO A) confirms a theoretical prediction. Br J Pharmacol 2007; 152: 946-951.