Insertion technique
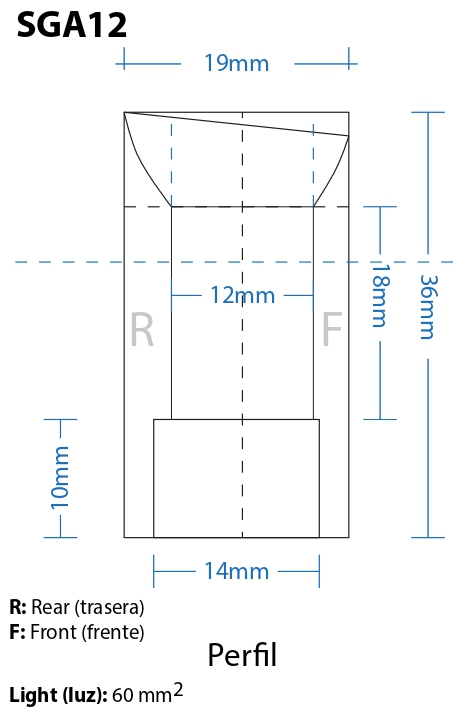
The length and diameter of the stenosis must be properly determined in order to select a stent of appropriate size: available in small or large. The area useful for ventilation is 40.6 mm² in the small model, and widens to 60 mm² in the large model.
The procedure is performed under general anesthesia. The basic introduction maneuvers are the same as those used for the rest of the straight intratracheal stents, with some variations detailed below.
A prior endosurgical treatment of the affected area may be necessary, in order to increase and adapt the diameter of the airway so the stent can be lodged.
For its implantation a tracheoscope or a prosthesis introducer may be used, inside which the stent is placed so that its widest, oval end is in the proximal position, since it will occupy the subglottic area, immediately below the vocal cords. The opposite end of the stent will be the distal one, since its final destination is the first tracheal portion.
Positioning
When introducing the stent into the tracheoscope or prosthesis loader, make sure that the plane of the stent marked “A” is “anterior”. Because the implant is subglottic, the end of the tracheoscope must not cross the vocal cords excessively, but rather remain insinuated between the two open cords.
From this position, push the stent with the prosthesis ejector rod until the stent leaves the tracheoscope through its distal end and lodges in the subglottis. The stent must not be pushed against the vocal cords. Position-adjustment maneuvers may be required and performed with an alligator forceps.
It is preferable that the final distance between the vocal cords and the stent be equal to or greater than 2 mm. Keep in mind that distances in the airway are difficult to estimate, since the length of the organ may vary between the standing and lying positions. The recovery of muscle tone after anesthesia adds an additional difficulty in determining anatomical distances. Transient changes in tracheal length may also occur, due to prior dilation maneuvers performed with rigid instruments on the organ.
Some or all of these circumstances may be present in laryngotracheal lumen reconstruction and implantation procedures, and the precautions that their nature requires must be taken. What is proposed here proceeds from what is known at the time of this revision and does not invalidate or contradict other implantation and removal modalities that, by their usefulness or experience, each operator deems preferable.
Removal technique
The Subglottic Artemic stent can be removed with an alligator-type forceps and with the aid of a tracheoscope or a laryngoscope.