Available dimensions
The Stening® High Pressure is offered with a 16.25 mm diameter in six lengths (30, 40, 50, 60, 70 and 75 mm).
| Code | Diameter | Length |
|---|
| SAP16-30 | 16.25 mm | 30 mm |
| SAP16-40 | 16.25 mm | 40 mm |
| SAP16-50 | 16.25 mm | 50 mm |
| SAP16-60 | 16.25 mm | 60 mm |
| SAP16-70 | 16.25 mm | 70 mm |
| SAP16-75 | 16.25 mm | 75 mm |
Measurements expressed in millimeters (diameter and length). The greater wall thickness reduces the area available for airflow. For specific inquiries about sizes, instruments, bronchoscopes or introducers, contact us at (+54) 11 4553-5070 or (+54) 11 4551-2333.
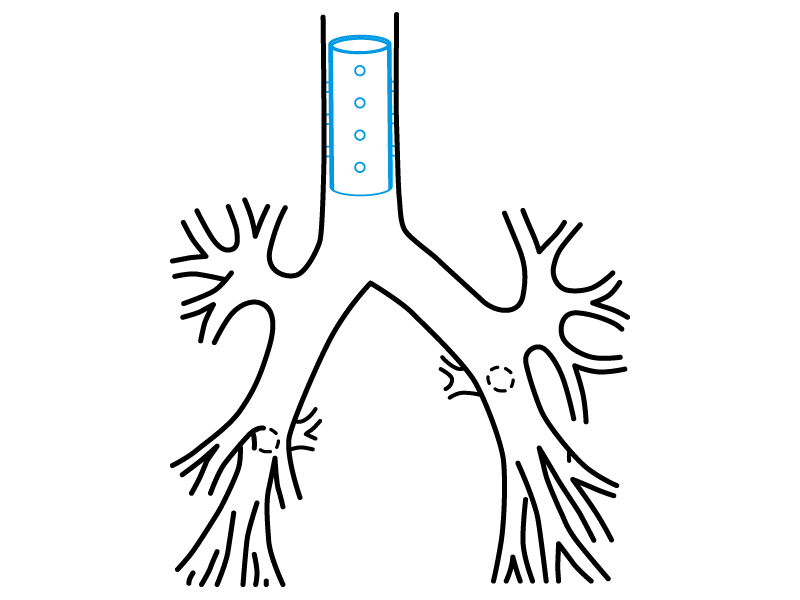
Insertion technique
The procedure is performed under general anesthesia. The implant can be carried out directly through the working channel of the tracheoscope.
The length and diameter of the area to be covered with the stent must be properly established. A simple method to determine the length of the affected area is to mark the tracheoscope when its tip reaches the end of the lesion, and to repeat the marking after withdrawing it back to the beginning of the lesion. The diameter of the trachea must be estimated by comparison with the known diameter of the endoscope used.
Implantation method
Every suggestion offered by the manufacturer is subordinate to the knowledge and experience of the expert professional—that is, to their know-how—in determining the best way to proceed in order to achieve the best result.
To this end, Stening considers and suggests that:
- The stent may only be loaded directly into the tracheoscope.
- Antegrade implantation should preferably be performed.
Antegrade implantation method
Stop the tracheoscope containing the prosthesis 5 mm before the lesion to be treated, and slowly press the ejector plunger. In this way, the prosthesis will be expelled toward the affected trachea.
Correction of the stent position
The stent may require additional maneuvers in order to correct or adjust its final position. It is preferable to correct a stent that has been installed beyond the desired position than the opposite, since it is highly inconvenient to advance a prosthesis that has been released “before” the affected area.
To move a stent in a proximal direction, it can be grasped by its edge and pulled.
Removal technique
Intubation is performed with a tracheoscope. The high-pressure stent must be grasped by its edge with an alligator forceps, firmly. The forceps is rotated about 360° so that the stent folds. Then the forceps is pulled, extracting the prosthesis together with the tracheoscope.
The proximal end of the stent must be introduced inside the tracheoscope. With this maneuver, the vocal cords are protected during extraction. Other methods of implantation and removal are possible depending on the operator’s experience and preferences.
Special considerations for the Stening® High Pressure
The comparative tests expressed above clearly show that the compression tolerance of a high-pressure stent is slightly more than double that of a classic stent. Therefore, placing the prosthesis in the introducer may be difficult; it is then recommended to apply it directly through the tracheoscope.
Except in very firm tracheal compressions, complete expansion of the stent will occur within a short time. Removal of the prosthesis should be performed only once the causes of the compressive phenomenon have disappeared. Proceed as in all cases of straight stent removal and use a strong forceps, since the stent will be strong as well.
The special indications for the use of a high-pressure stent must be discussed and agreed upon by consensus. Severe tracheal compressive phenomena have different etiologies and may be accompanied by superior vena cava syndrome or other serious disorders of intrathoracic venous circulatory difficulty. In these cases, as well as in the presence of mediastinal syndrome, it should be considered to anticipate the application of a vascular stent prior to the implantation of a tracheal stent. The high-pressure stent must be used only by expert bronchoscopists.