Available dimensions
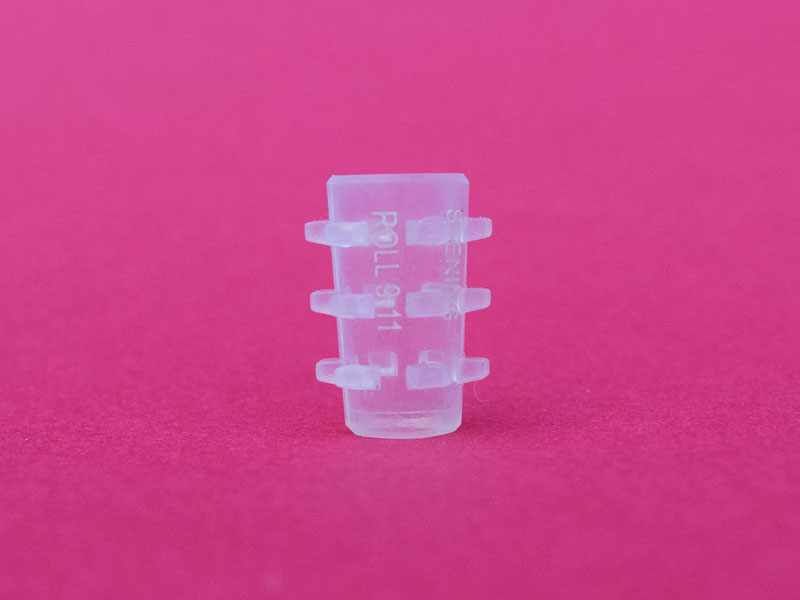
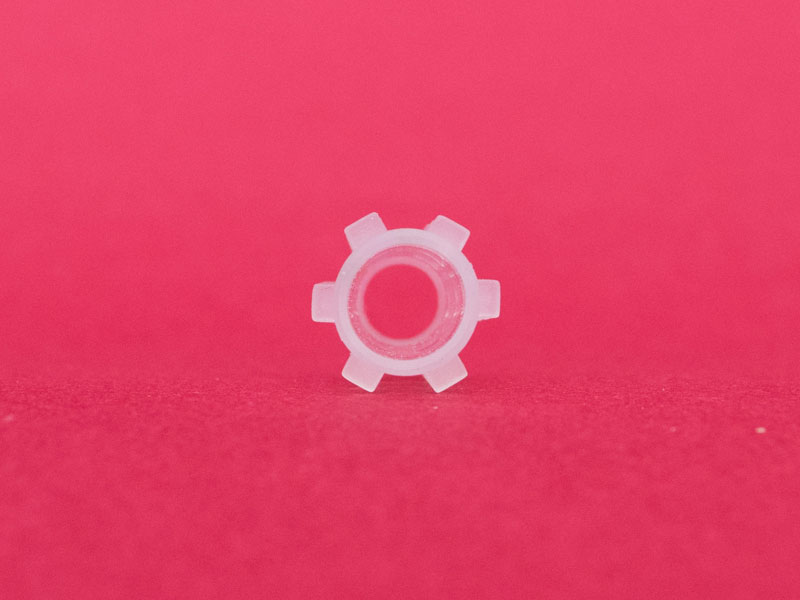
The Stening® Roll is offered in three sizes with differentiated external distal and proximal diameters, which reproduce the taper of the bronchus to be treated.
Measurements in millimeters. The distal (A) and proximal (B) diameters correspond to the ends of the stent and the length (C) to its total span. For specific inquiries about instruments, bronchoscopes or introducers, contact us at (+54) 11 4553-5070 or (+54) 11 4551-2333.
Insertion technique
As always, and as in the foregoing, treatment is carried out under general anesthesia. Owing to its small dimensions, the implant of this type of prosthesis can be performed directly through the working channel of a thin bronchoscope, 7 mm in diameter or similar, or by using a conventional introducer for silicone prostheses. The airway is accessed with a rigid endoscope.
Antegrade implantation method
Stop the bronchoscope in front of the affected bronchial area. Introduce the small stent into the bronchoscope and push it to its distal end.
Correction of the stent position
The stent may require additional maneuvers in order to correct or adjust its final position. To move a stent in a proximal direction, it can be grasped by its edge and pulled gently. Such a small stent will be easy to move.
Removal technique
Intubation is performed with a rigid bronchoscope as appropriate. Easy to remove, the silicone stent must be grasped by its edge with a forceps. No rotation maneuver will be necessary to extract a ROLL stent.
Specific considerations for the Stening® Roll
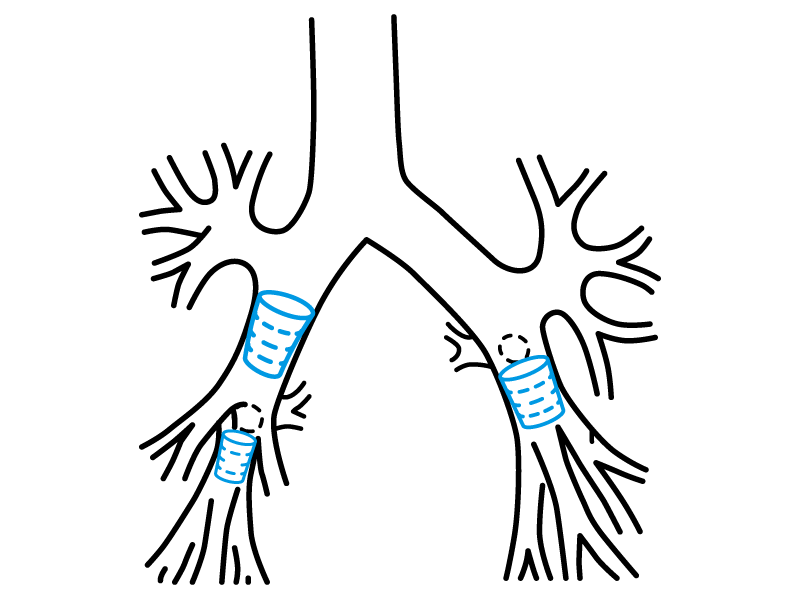
The division spurs of the basal segments stop the stent and prevent its implantation in an undesired site. For implantation, all sizes of the Stening® Roll can be introduced into a number 8 bronchoscope or one of larger diameter. Once the endoscope is positioned near the bronchus intermedius or lower lobe bronchus as the case may be, introduce the previously lubricated and folded Stening® Roll through the end of the bronchoscope, then push it with the bronchoscopy forceps until it leaves the endoscope at its opposite end and is thus lodged in the bronchus. A standard stent loader and its pusher for a number 8 or 9 bronchoscope, or whichever you prefer, may also be used.
When loading the stent into the bronchoscope, remember that the widest end of the Roll (letter “B” in the diagram) must be placed in the proximal position so that it faces the bronchoscopist. Conversely, the narrowest end will occupy the distal position. Removal is simple compared to that of a conventional stent owing to the small dimensions of the Stening® Roll.
The Stening® Roll can be trimmed at its end to fit the length of the bronchus in which it is implanted. Make the cut at its proximal end, since this end does not face any bronchial spur during respiratory dynamics. Implanting a stent in the common trunk of the lower lobe may result in occlusion of the entrance of the apical segment; the physician must weigh the benefits of restoring ventilation of the basal segments despite the loss of the apical segment of the lower lobe, when it is not already affected by the neoplastic disease.